
Noa Scheinowitz¹, Dr. Saar Lanir-Azaria¹
1 Dormotech Medical
Background
Obstructive sleep apnea (OSA) is a highly heterogeneous disorder characterized by dynamic upper-airway collapse during sleep, with disease expression strongly modulated by sleep posture. Among the recognized phenotypic subtypes, positional obstructive sleep apnea (POSA) represents one of the most prevalent and clinically relevant forms, wherein respiratory instability is markedly exacerbated during supine sleep relative to lateral positions (Cartwright, 1984; Mador et al., 2005). Supine posture has been consistently associated with increased upper-airway collapsibility, augmented pharyngeal tissue displacement, reduced lung volume, and impaired neuromuscular compensation, collectively promoting greater respiratory event frequency, prolonged airflow limitation, and more severe nocturnal hypoxemia (Joosten et al., 2014).
The clinical relevance of positional dependency extends beyond simple variation in apnea–hypopnea index (AHI). Positional changes substantially influence the physiological burden of disease, including oxygen desaturation dynamics, autonomic activation, sleep fragmentation, and cumulative hypoxic stress. Consequently, characterization of sleep posture has become an integral component of contemporary sleep testing and OSA phenotyping. Current polysomnography (PSG) and home sleep testing (HST) systems routinely incorporate body-position monitoring, typically through a single trunk-mounted accelerometer enabling classification into broad positional categories such as supine, prone, and lateral sleep. While this approach provides clinically valuable information regarding posture-dependent respiratory worsening, it remains anatomically and physiologically reductive, as it assumes torso orientation adequately represents upper-airway configuration throughout sleep.
This assumption likely represents a major limitation of current positional sleep analysis. Conventional positional monitoring does not directly quantify head or cervical orientation, despite the fact that upper-airway patency is fundamentally governed by cranio-cervical mechanics rather than trunk posture alone. Head rotation and neck positioning may independently alter pharyngeal geometry, tissue tension, mandibular alignment, and gravitational loading of upper-airway structures, thereby modulating airway collapsibility even when body posture remains unchanged. Indeed, prior physiological investigations demonstrated that lateral head rotation during supine sleep can significantly attenuate OSA severity independent of trunk position (Zhu et al., 2017). Similarly, Tate et al. (2020) identified the absence of head-position assessment as a critical technological limitation in currently available positional monitoring methodologies and emphasized the need for integrated positional characterization approaches capable of differentiating head and body orientation.
Despite these observations, head-position assessment has not been systematically integrated into standard clinical sleep evaluation, and the physiological significance of head orientation during sleep remains insufficiently characterized. Several unresolved questions therefore persist. It remains unclear whether continuous head-position monitoring provides clinically meaningful information beyond conventional body-position assessment alone; whether specific head orientations are associated with measurable reductions in respiratory event burden or hypoxic stress; and whether combined body–head positional phenotyping may improve identification and characterization of posture-dependent OSA subtypes. Furthermore, while previous positional studies primarily focused on AHI-based outcomes, considerably less attention has been directed toward the relationship between head orientation and physiological severity metrics such as hypoxic burden, which may better reflect the cumulative biological consequences of sleep-disordered breathing.
The Dormotech DormoVisionX platform enables synchronized continuous monitoring of both body and head orientation throughout sleep using independent triaxial accelerometer systems. This capability allows high-resolution characterization of cranio-cervical and torso positional dynamics during sleep and provides a unique opportunity to investigate whether combined body–head positional assessment yields additional physiological and clinical insight beyond conventional positional monitoring paradigms. Accordingly, the present study aimed to explore the relationship between integrated body and head orientation, respiratory event distribution, and positional hypoxic burden during sleep, while evaluating the potential contribution of combined positional monitoring to the characterization of positional OSA.
Methods
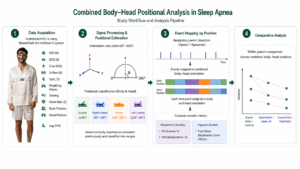
A single-patient exploratory physiological analysis was conducted using a clinical unattended Home Sleep Apnea Test (HST-II) acquired with the DormoVisionX system (Dormotech Medical), which continuously acquired physiological and respiratory signals including frontal EEG channels, bilateral EOG, chin and limb EMG, airflow signals, thoracoabdominal respiratory effort, pulse oximetry (SpO₂), heart rate, snoring, body position, and head position, as illustrated in the study workflow presented in Figure 1. The selected patient demonstrated clinically significant positional obstructive sleep apnea with substantial positional variability throughout the recording and predominance of obstructive respiratory events.
Continuous body and head orientation were derived from synchronized triaxial accelerometer recordings obtained from the torso and head units. Positional angles were calculated from normalized acceleration vectors and transformed into continuous angular representations across the 0°–360° plane. Sleep posture was subsequently categorized into supine, right lateral, prone, and left lateral orientations according to predefined angular thresholds.
Respiratory events were extracted from the annotated sleep recording and mapped to the corresponding positional orientation throughout the study. Positional respiratory indices were calculated by normalizing event frequency to cumulative time spent within each positional range. In parallel, positional hypoxic burden was quantified from synchronized SpO₂ recordings by calculating the cumulative magnitude and duration of oxygen desaturation below the estimated baseline saturation curve for each positional state.
The analysis focused specifically on evaluating respiratory severity across synchronized combinations of body and head orientation, with particular emphasis on respiratory burden during persistent supine body posture combined with varying head positions.
Results
Figure 2 presents positional hypoxic burden analysis derived from the patient recording. Polar positional maps demonstrated a marked positional dependency of physiological respiratory burden during sleep. Body-position analysis revealed that the majority of cumulative hypoxic burden occurred during supine body posture, consistent with a positional OSA phenotype. However, respiratory severity was not uniformly distributed across the supine body-position category. Combined body–head positional analysis demonstrated that respiratory burden varied substantially according to head orientation, even while body posture remained persistently supine.

The lowest respiratory severity and hypoxic burden were observed when the patient remained in supine body posture while the head was oriented upward in a neutral aligned position. In contrast, respiratory severity markedly worsened when the head deviated laterally while body posture remained supine. Both leftward and rightward head rotation during supine body positioning were associated with greater respiratory event burden and cumulative hypoxic stress.
This positional relationship is illustrated in the combined body–head heatmap shown in Figure 2B, demonstrating concentration of respiratory burden within specific synchronized positional states rather than uniformly across all supine sleep.
Discussion
The primary objective of this physiological case analysis was to explore whether combined assessment of body and head orientation provides additional insight into positional obstructive sleep apnea beyond conventional body-position monitoring alone. Specifically, the analysis aimed to evaluate whether variability in head orientation during otherwise stable body posture is associated with measurable differences in respiratory severity and positional hypoxic burden.
The findings demonstrated that respiratory severity during supine sleep was strongly modulated by concurrent head orientation. Although the patient remained predominantly in supine body posture throughout large portions of the recording, respiratory burden was not uniformly distributed across all supine sleep states. Instead, synchronized body–head positional analysis revealed substantial variability in both respiratory event severity and cumulative hypoxic burden according to head orientation.
Interestingly, the lowest respiratory severity was observed during neutral upward-facing head positioning, whereas lateral head deviation during persistent supine body posture was associated with substantially greater respiratory burden and hypoxic stress. These findings suggest that head and cervical orientation may independently influence upper-airway behavior even when trunk posture remains unchanged (Zhu et al., 2017).
From a mechanistic perspective, these observations are physiologically plausible. Upper-airway collapsibility is likely influenced more directly by cranio-cervical alignment, mandibular positioning, gravitational loading of pharyngeal tissues, and neck posture than by torso orientation alone (Joosten et al., 2014). Alterations in head orientation may therefore substantially modify upper-airway geometry and airway stability despite unchanged body position.
These findings further highlight a potential limitation of current positional monitoring approaches routinely used in clinical sleep medicine. Standard PSG and HST systems typically classify posture using a single trunk-mounted sensor, thereby assuming that body orientation adequately reflects airway-related positional physiology. However, the present observations suggest that substantial physiological variability may exist within the same conventional body-position category depending on concurrent head orientation (Tate et al., 2020).
Importantly, the positional relationships observed in this patient differ from some previously described positional patterns in the literature, emphasizing the potential complexity and patient-specific nature of cranio-cervical contributions to airway physiology during sleep. This further supports the need for individualized positional characterization rather than reliance on simplified trunk-position classification alone.
From a clinical perspective, incorporation of synchronized head-position monitoring may improve phenotypic characterization of positional OSA and potentially refine identification of patients who could benefit from targeted positional interventions. These observations may also have implications for future positional therapy strategies focused not only on trunk posture but also on head and cervical orientation during sleep.
Several limitations should be acknowledged. First, this report represents a single-patient exploratory physiological analysis and was not designed to establish causal relationships between head orientation and OSA severity. Second, positional classification relied on accelerometer-derived angular estimation rather than direct anatomical imaging of cervical posture or airway configuration. Finally, larger studies will be required to determine the reproducibility, prevalence, and clinical significance of these positional effects across broader OSA populations.
Nevertheless, this case demonstrates the potential physiological value of integrated body–head positional assessment during sleep and highlights the possibility that conventional trunk-based positional monitoring may incompletely capture clinically relevant positional airway dynamics.
References
Cartwright RD. Effect of sleep position on sleep apnea severity. Sleep. 1984;7(2):110-114.
Joosten SA, O’Driscoll DM, Berger PJ, Hamilton GS. Supine position related obstructive sleep apnea in adults: pathogenesis and treatment. Sleep Med Rev. 2014;18(1):7-17. doi:10.1016/j.smrv.2013.01.002
Mador MJ, Kufel TJ, Magalang UJ, Rajesh SK, Watwe V, Grant BJ. Prevalence of positional sleep apnea in patients undergoing polysomnography. Chest. 2005;128(4):2130-2137. doi:10.1378/chest.128.4.2130
Tate A, Walsh J, Kurup V, et al. An emerging technology for the identification and characterization of postural-dependent obstructive sleep apnea. J Clin Sleep Med. 2020;16(2):309-318. doi:10.5664/jcsm.8178
Zhu K, Bradley TD, Patel M, Alshaer H. Influence of head position on obstructive sleep apnea severity. Sleep Breath. 2017;21(4):821-828. doi:10.1007/s11325-017-1495-2


